Lecture Notes
A really common chief complaint in the ED is Back Pain.
Like all chief complaints, the first things we need to do is develop a critical differential diagnosis. For back pain this includes:
- Cauda Equina
- Acute cord compression from traumatic/pathologic fracture
- Epidural abscess
- Epidural hematoma
- Abdominal Aortic Aneurysm
So let's review how each one of these critical differential diagnosis present:
Cauda Equina: The patient may have a history of bowel or bladder incontinence or retention. Saddle anesthesia and diminished rectal tone may be present on physical exam. The urinary incontinence that is described occurs because the patient can no longer sense his or her bladder becoming distended with urine. As a result the pressures inside the bladder overwhelm the urethral sphincters and lead to a constant dribbling of urine.
Acute cord compression: This occurs secondary to traumatic or pathologic fractures. It is important to ask the patient whether there has been a traumatic event prior to the presentation. Patients reporting significant weight loss may have a malignant process. Metastatic lesions to the spine are susceptible to atraumatic/pathologic fractures. For acute cord compression, the most sensitive physical exam finding will be sensory level cutoff. As a reminder, the nipple line correlates with the T4 dermatome and the umbilicus correlates with the T10 dermatome. Always check for a sensory level cutoff on patients presenting with back pain.
Epidural Abscess: The classic triad is fever, midline point tenderness, and a social history of IV drug use. Studies have shown that the absence of this triad is not sensitive enough to absolutely rule out epidural abscess. However, if the patient has all three features, epidural abscess should be high on your differential.
Epidural Hematoma: This will present in patients who are anticoagulated.
Abdominal aortic aneurysm (AAA): AAA generally occurs in older patients. On exam, the patient will be hypotensive and will possibly have a pulsatile abdominal mass. Remember that the aorta is a retroperitoneal structure. As a result, AAA will present with back pain instead of the classic guarding, rebound, and rigidity that is seen in appendicitis, diverticulitis, or other processes that irritate the peritoneal lining.
The Work Up
If you have a high concern for one of the critical differentials you should jump straight to MRI if possible. For older patients, a bedside point of care ultrasound should be performed to ensure that the patient does not have an AAA rupture.
Treatment
If you have ruled out all of the dangerous causes for back pain and have determined that the patient's symptoms are caused by a benign process such as sciatica, you can begin treating the patient’s pain with an NSAID such as toradol (provided that the patient does not have kidney issues) and a muscle relaxer such as baclofen or flexeril. Notice in our treatment algorithm we do not include opiates. We are trying to treat the underlying cause of the pain, which is inflammation and muscle spasm instead of simply masking the pain with opiates.

ddxof.com Algorithm for Back Pain
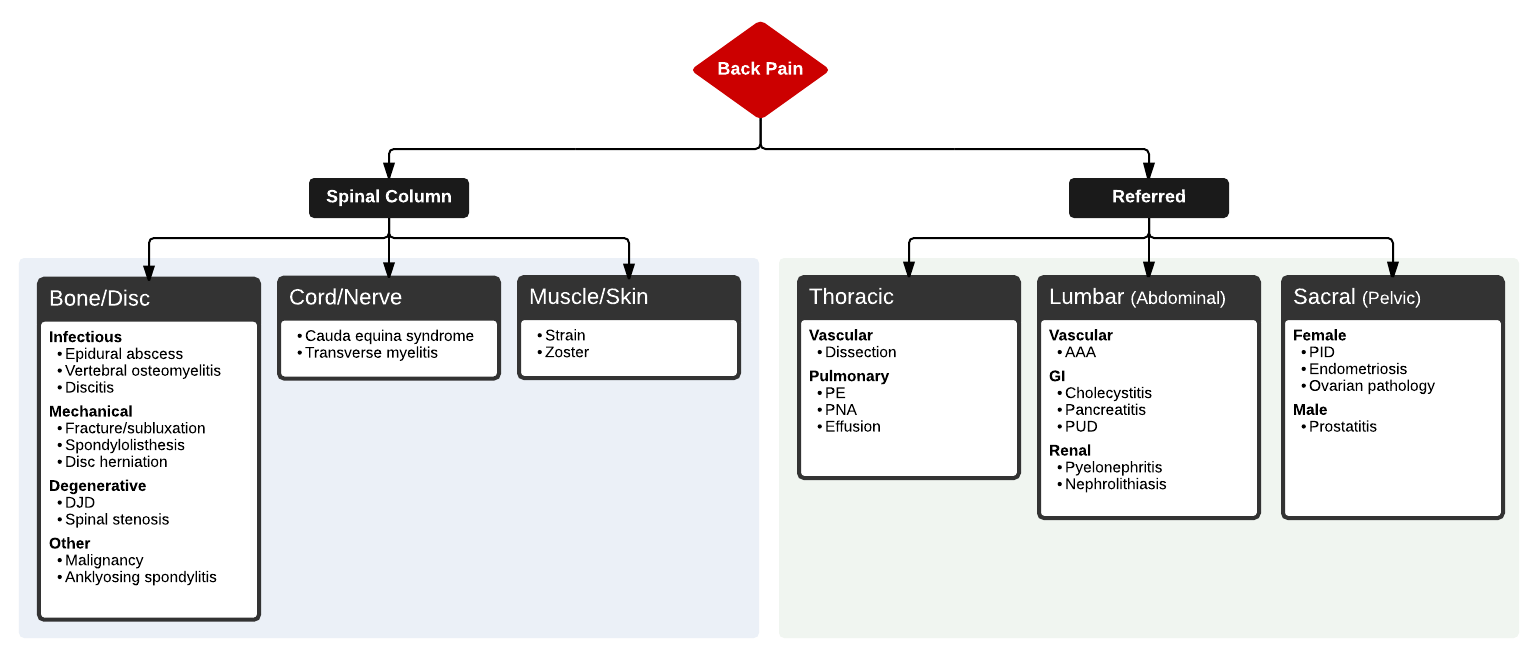
Full ddxof.com article and algorithm on Back Pain can be found at https://ddxof.com/back-pain/
Subscribe to the EM Ed by entering your email in the subscription box below. Don't rely on Facebook to get notifications for new posts. We only email when a new post is published. No spam. If you are reading this on your phone, just keep scrolling down to get to the Subscribe box.
Give us some love by sharing the EM Ed with people you think would like it. Post the lecture on social media. Like and Follow our Facebook Page. Follow us on Twitter. Follow us on Instagram