2025 Guideline, Endorsed by the following professional societies:
American Academy of Family Physicians (AAFP)
American Academy of Neurology (AAN)
American Academy of Physician Associates (AAPA)
American Association of Nurse Practitioners (AANP)
American Association of Psychiatric Pharmacists (AAPP)
American College of Medical Toxicology (ACMT)
American College of Obstetricians and Gynecologists (ACOG)
American Geriatrics Society (AGS)
American Psychiatric Association (APA)
American Society of Addiction Medicine (ASAM)
Overview
In the USA, 24 million people reported BZD use; 50% who were dispensed oral medication received >=2 months supply.
2023 National Survey on Drug Use and Health (NSDUH): 15% reporting BZD misuse
Abrupt discontinuation of regularly used BZDs can lead to serious and life-threatening withdrawal
Relevance to Emergency Departments: Patients presenting in withdrawal from nonprescribed BZDs, not tolerating a taper from their regular prescriber, or have lost access to their BZD prescription.
General Considerations
Medication dosage should be tapered gradually (weeks to months) under clinical supervision; sometimes it can take months to years to fully taper off
Considerations include level of care, tapering strategies, withdrawal management
Note there is a paucity of evidence regarding benzodiazepine tapering, so guidelines are based on clinical consensus
Tapering indicated when risks of continuing BZD outweighs benefits
Sometimes, the goal is to just taper to a lower dose where the risks are now lowered
Note that there are some indications for long term BZD use: severe treatment resistant GAD, bipolar spectrum disorders, complex seizures, spasticity, REM sleep disorder, restless legs syndrome, catatonia.
Most tapers can be completed outpatient, but consider withdrawal risks, social circumstances, concurrent medical and mental health conditions as possible factors for inpatient treatment
Withdrawal
Characterized by anxiety, irritability, insomnia, tremors, malaise, progressing to seizures/delirium
Protracted withdrawal: symptoms can persist for months/years after BZD discontinuation
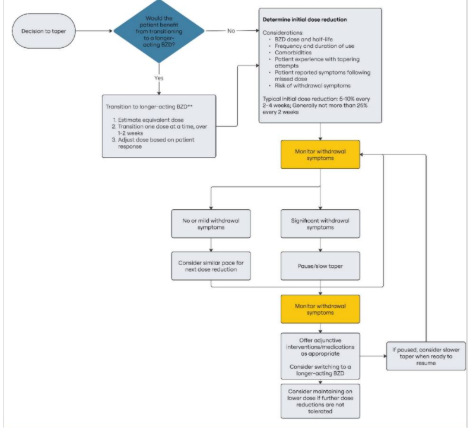
Tapering
Heterogeneity in patient response to tapering:
Some individuals on high dose long term benzodiazepines can tolerate relatively quick tapers (e.g. decrease 25% every 2-4 weeks), whereas some individuals on low doses for shorter period of time experience significant withdrawal, even with slow taper (e.g. 5% every 4 weeks).
Therefore, guideline recommends patient centered approach – start slow and adjust based on response, and offer options.
Consider transition to a comparable dose of longer acting BZD medication (e.g. diazepam, clonazepam) for the taper: https://www.mdcalc.com/calc/10091/benzodiazepine-conversion-calculator
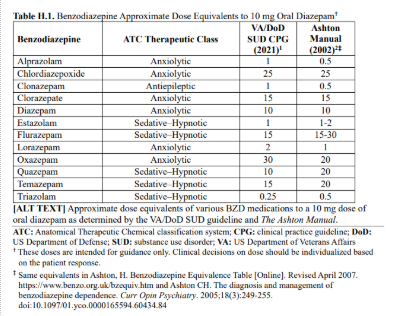
Lorazepam in those with severe hepatic impairment
General Strategy: Dose reduction of 5-10% every 2-4 weeks; do not exceed 25% every 2 weeks.
References:
1. Brunner E, Chen CYA, Klein T, et al. Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits. J Gen Intern Med. 2025;40(12):2814-2859. doi:10.1007/s11606-025-09499-2
2. Soyka M. Treatment of Benzodiazepine Dependence. New England Journal of Medicine. 2017;376(12):1147-1157. doi:10.1056/NEJMra1611832